
Overview of Little League Shoulder
Little league shoulder is a very common diagnosis in young baseball players experiencing shoulder pain. Approximately 10% of all pediatric injuries are related to throwing sports. The injury could occur to any child with open growth plates, but is most common in ages 11-15. Generally, the injury responds very well to conservative management with over 90% of players returning to baseball. There are a smaller percentage of players that return to baseball, but change positions and no longer pitch. Unfortunately, the injury has a relatively high rate of recurrence with around 19% of players having setbacks with recurrent shoulder pain.
Little league shoulder is most common in baseball players, but can be present in tennis players, volleyball players and other overhead athletes.
Anatomy of Little League Shoulder
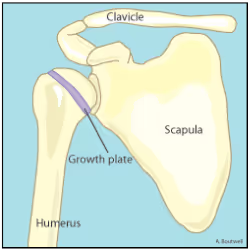
Little league shoulder is an overuse injury to the growth plate or physis of the upper arm bone (called the humerus). Essentially, stress in the arm tends to injure the weakest link of the body. In older players, the bones are hard and relatively resistant to injury, therefore older players tend to deal with more soft tissue injuries like the labrum, the muscles and tendons of the shoulder. With younger players, the growth plate is made out of soft cartilage and is the “weak point” of the shoulder.
In little league shoulder, the cartilage of the growth plate undergoes a series of microtraumas from the repeated torsion of throwing a baseball, with pitching being the most stressful throwing motion in baseball. These small series of traumas to the growth plate can cause a widening of the growth plate and eventually permanent damage to the growth plate if it is not addressed and managed properly.
Causes of Little League Shoulder
Little league shoulder is caused by overuse of the arm through throwing. It is more common in young pitchers than in young position players. It can be caused by too many throws in a day or week, playing too many games, poor pitching mechanics, and not taking time off from throwing in young players.
The largest correlation with increased risk of shoulder pain with throwing in 9-14-year-olds was increased number of pitches in a game. Once a player is above 75 pitches/game, they are increasingly more likely to develop shoulder pain with each pitch thrown. Throwing more than 370 pitches per season also statistically increased the risk of developing shoulder pain in 9-14-year-olds.
When examining pitching mechanics there are known deviations that cause increased stress on the shoulder and elbow, like forearm climb and flying open. However, there has not been a demonstrated relationship between one pitching mechanic flaw and development of little league shoulder.
Common Little League Shoulder Symptoms
The most common initial symptom of little league shoulder is shoulder pain while throwing or swinging a racquet. As the injury progresses, the player may develop pain with other activities like reaching overhead, lifting and carrying heavier objects.
The most common clinical finding is shoulder pain to palpation on the outside of the shoulder right over the front or back of the greater tuberosity of the humerus.
Diagnosis of Little League Shoulder
Diagnosis is typically a combination of patient symptoms, clinical examination, and confirmed by x-ray that will show widening of the growth plate in the upper arm bone in 99% of reported cases.
The x-ray can also be important to rule out other more significant injuries to the growth plate like cysts or a fracture to the growth plate.

Little League Shoulder Complications
Typically little league shoulder will resolve with conservative management and no need for surgical intervention. The majority of players are able to return to baseball and pitching within 3-6 months.
The most common complication of little league shoulder is a fracture through the growth plate called a Salter-Harris fracture, which would be seen on an x-ray. Any permanent damage to the growth plate has the potential to affect the ongoing growth and boney development of the arm.
Prevention of Little League Shoulder
While no injury can ever be completely prevented, one of the large keys in youth baseball players is managing workload. The most significant correlation to injuries is specifically related to pitch counts, both within a day and over the course of the season.
In 9-14 year old players, it appears to be protective to limit players to around 75 pitches/game or less and to limit the number of pitches in 1 season to 370 pitches or less. Additionally, in youth pitchers it appears to be protective to take 1 season/year off of throwing.
Major League Baseball and USA Baseball have worked together to develop the “Pitch Smart Guidelines.” While there is no perfect throwing plan for every individual, this is a great resource as a starting point for players, families and coaches to manage pitching workloads in youth pitchers.
Please note that after a downtime from throwing, it is important to follow a structured build up program to gradually prepare the arm for the stress of pitching. A Major League pitcher put together a preseason throwing program that is a perfect resource for younger throwers starting to build a consistent routine going into each season or beginning to throw again after a period of time off.
Recovering From Little Leaguer Shoulder:
In most cases, little leaguer shoulder is managed conservatively with no medical intervention necessary. It requires a period of relative rest, and often physical therapy to help with activity modification, addressing physical deficits and assisting with managing a gradual return-to-sport.
Treatment Plan for Little League Shoulder
Initially, little league shoulder requires complete rest from throwing for ~4-12 weeks. During this time the player is able to continue with other athletic activities, as long as they are pain free. For example, many players are able to swing a bat without pain and would be able to continue competing with their team as a designated hitter and base runner.
This initial time period with restricted throwing is a perfect time to address other physical deficits. For example, some players will have a limited shoulder range of motion or decreased shoulder strength that can be addressed through physical therapy and an exercise program. Additionally, it is a great time to work on improving the kinetic chain: addressing core control, thoracic spine mobility and lower body control. Doing so during this phase of rehabilitation can help reduce stress on the arm when the player returns to throwing.
Players experiencing little league shoulder are often able to continue with lower body strength training and conditioning with minimal modifications.
The primary criteria for progression into the return-to-throwing phase of the rehab is decreased shoulder pain. We recommend players have full and pain-free range of motion, full and pain-free upper body lifting, and no pain with 1- and 2-hand upper body plyometrics before progressing to a throwing program. Some doctors recommend a repeat x-ray prior to beginning a throwing program, but closure of the growth plates on x-ray is not a requirement to begin a throwing program as long as symptoms have resolved.
Return-To-Throwing
The following is the criteria for a player to be considered ready to begin a return-to-throwing program:
- Pain free range of motion
- No tenderness to palpation on the outside of the shoulder
- Equal and pain free shoulder strength
- Return to upper body strength training with no pain
- Completion of 1-hand and 2-hand upper body plyometrics with no pain
If a player has met all of the above, they are ready to begin progressions towards throwing. Following an extended layoff from throwing, the player needs to go through a gradual throwing program. Typically, we recommend the player goes through a long toss progression of equal length as their time away from throwing. So if they took 6 weeks off of throwing to allow symptoms to resolve, they would complete a 6 week long toss program.
Following the long toss program, position players are cleared to fully return to game play.
Pitchers then need to go through a mound progression, including bullpens and live at bats prior to returning to competition on the mound. Typically, this begins with 20-pitch bullpens and progresses to 40-pitch bullpens and live at bat sessions. Once the player completes the mound progression, we recommend 1-2 innings of pitching in their first return to competition.
Little League Shoulder Protocol and Exercises
Early Phase:
The early phase of little league shoulder rehabilitation will be the most variable based on the symptoms of the player. Everything in this phase should be guided by symptoms and remain pain free.
The focus of this phase is ensuring the athlete has full pain-free range of motion, ability to perform low threshold shoulder strength exercises and is able to reintegrate into normal upper extremity strength training without pain.
Examples of exercises that would be included in this phase:
- Foam roll lat
- Lacrosse posterior shoulder
- Lumbar locked lat breathing
- Band External Rotation Walkouts
- Band T’s
- Forearm Circuit
Intermediate Phase:
This phase is focused on regaining upper body strength. The athlete will continue to work to maintain full range of motion, and will incorporate progressively heavier loads in their strength exercises. At the end of this phase, you will also begin to incorporate upper body plyometric exercises to start preparing the arm for throwing. In order to progress to the next phase you need to be able to perform a series of 1- and 2-arm plyometric exercises 3 days/week without shoulder pain.
Examples of exercises that would be included in this phase:
- Push Ups
- Dumbbell Rows
- 90/90 External/Internal rotation
- TRX T’s
- Med Ball Chest Pass
- Med Ball Overhead Throw
- Wall Dribble
Return-to-Throwing Phase:
This phase is largely dictated by the throwing program. Each throwing program should be unique to each athlete, but typically begins throwing 3 days/week and progresses gradually to prepare the arm for the required practice and game schedule.
The athlete will continue with many of the exercises and progressions from the last phase with a focus on returning to full performance.
Example exercises:
- Ball Drops
- Ball flips
- Reverse Throws
- Arm Bar
Conclusion:
Little league shoulder is a common upper extremity injury for youth baseball players. While it is a setback that typically results in a significant period of forced rest from throwing, the long term outcomes from this injury are good. The vast majority of players return to baseball and are even able to return to pitching with no need for surgery or significant medical intervention. Unfortunately, it does have a high recurrence rate with about 20% of players dealing with a second bout of little league shoulder during their career.
It is crucial to the rehab process to go through a thorough return-to-throwing program, learn about proper workload management and develop an arm care routine to help keep your arm healthy for the long run!
References:
- Bednar, E. Dimitra, et al. “Diagnosis and Management of Little League Shoulder: A Systematic Review.” Orthopaedic Journal of Sports Medicine 9.7 (2021): 23259671211017563.
- Sabick, Michelle B., et al. “Biomechanics of the shoulder in youth baseball pitchers: implications for the development of proximal humeral epiphysiolysis and humeral retrotorsion.” The American journal of sports medicine 33.11 (2005): 1716-1722.
- https://www.mlb.com/pitch-smart/pitching-guidelines

